概述
开颅术
开颅术
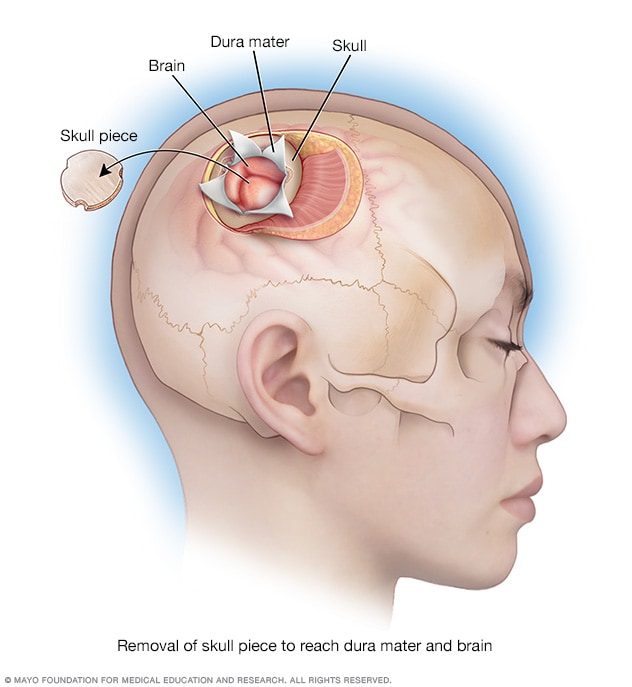
在开颅术中,切除一块颅骨,露出覆盖大脑的坚硬组织(即硬脑膜)和大脑。
开颅术需要移除一部分颅骨,以进行脑部手术。可能为了提取脑组织样本或者治疗影响脑部的状况或损伤而行开颅术。
该手术用于治疗脑肿瘤、脑出血、血凝块或癫痫发作。进行该手术还可以治疗脑血管膨胀(称为脑动脉瘤)。或者,开颅术可以治疗不规则形成的血管(称为血管畸形)。如果损伤或卒中引起脑水胀,开颅术可以释放脑部压力。
开颅术有多种类型。所用开颅术的类型取决于移除颅骨哪个区域进行治疗。手术类型包括:
Craniotomy types
There are several types of craniotomies. The type of craniotomy that is used depends on which area of the skull is removed for treatment. Craniotomy types include:
- Bifrontal craniotomy. A surgeon removes part of the front of the skull behind the hairline. This may be done to treat a brain aneurysm.
- Supraorbital craniotomy. This surgery involves removing an area of the skull just above the eye socket. The opening is usually made through a short incision hidden in the eyebrow, which is why it is sometimes called an eyebrow craniotomy. This approach allows surgeons to reach the front of the brain and skull base to treat conditions such as brain tumors or aneurysms, while keeping the scar less visible and limiting the size of the bone opening.
-
Pterional craniotomy. A surgeon removes part of the skull on the side of the head in front of and above the ear. Another name for this type of surgery is frontotemporal craniotomy.
Pterional craniotomy can be done to treat brain aneurysms, brain tumors, blood clots, epilepsy and arteriovenous malformations. Sometimes a pterional keyhole craniotomy is done, which removes a smaller area of the skull.
- Suboccipital craniotomy. A surgeon removes a piece of the base of the skull in the lower area at the back of the head. This type of craniotomy is done to treat a condition where brain tissue extends into the spinal canal, known as a Chiari malformation. It also can treat brain tumors, aneurysms, cavernous malformations and arteriovenous malformations.
- Retrosigmoid keyhole craniotomy. A small hole is cut in the skull behind the ear. This type of surgery may be used to treat an aneurysm. It also may be used to treat a noncancerous tumor on the nerve leading from the inner ear to the brain. This type of tumor is known as an acoustic neuroma or a vestibular schwannoma. A retrosigmoid keyhole craniotomy is a type of suboccipital craniotomy. It's a less invasive version that uses a smaller opening behind the ear to reach the tumor, which may reduce recovery time and side effects.
- Middle fossa craniotomy. The surgeon makes an opening in the skull just above the ear. This allows the surgeon to reach the middle part of the brain's base, called the middle cranial fossa. Surgeons often use this approach to remove smaller tumors or to treat problems in the inner ear canal and nearby bone.
- Far lateral approach. For this surgery, part of the skull behind the ear is removed. The surgeon uses a thin, flexible tube known as an endoscope to remove a tumor.
- Orbitozygomatic approach. The surgeon removes small parts of the eye socket and cheekbone for better access. It's used for complex tumors or blood vessel problems. This approach helps the surgeon reach deep or hard-to-access areas at the base of the skull. The approach reduces the need to move or press on brain tissue.
Variations on craniotomy surgery
Other procedures are similar to craniotomy, but they have a few differences in why and how they're done.
Craniectomy
A craniectomy is similar to a craniotomy, but the removed skull bone is not replaced at the end of the surgery. This is usually done in emergencies when the brain is swelling dangerously.
Why it's done
- After traumatic brain injury.
- After major stroke that blocks blood flow through the middle cerebral artery, one of the brain's major blood vessels.
- When very high pressure inside the skull doesn't get better with medicine or with a ventilator to help the person breathe.
Key points
- The piece of skull bone is either stored or discarded.
- It gives the brain room to swell safely without being squeezed.
- A second surgery called a cranioplasty may be needed later to repair the skull.
Cranioplasty
Cranioplasty is surgery to repair the shape of the skull, usually following a previous craniectomy. This repair typically uses the original piece of skull removed during the craniotomy. It may use artificial materials if the original piece of skull can't be used.
Why it's done
- To protect the brain by covering the opening in the skull.
- To restore the shape of the head.
- Sometimes, to help the brain work better, especially if symptoms appeared after the skull piece was removed.
Key points
- This surgery is done to repair the skull, not to treat the original brain condition.
- It's usually a planned procedure that happens after the brain swelling has gone down.
Burr hole procedure
A burr hole is a small hole drilled into the skull without removing a bone flap to treat or diagnose brain conditions.
Why it's done
- To drain old blood that has built up on the surface of the brain.
- To insert a tube that helps remove extra fluid from the brain, known as a ventricular drain.
- To take a small sample of brain tissue for testing, called a biopsy.
- To reach fluid-filled spaces in the brain when placing a device that helps drain excess fluid, known as a shunt.
Key points
- It is a minimally invasive procedure, meaning it uses a small opening and causes less disruption to the skull and brain.
- No large piece of bone is removed — only a small hole is made.
- Sometimes, it can be done with local anesthesia, so the person stays awake but the area is numbed.
目的
可以进行开颅术获取脑组织样本进行检测。或者可以进行开颅术治疗影响脑部的疾病。
开颅术是用于切除脑肿瘤的最常见的手术。脑肿瘤可能会对颅骨造成压力或引起癫痫发作或其他症状。开颅术期间移除一块颅骨使外科医生可以进入脑内切除肿瘤。有时始于身体其他部位的癌症扩散至脑部,则需要进行开颅术。
如果脑出血(称为出血)或者需要清除脑内的血凝块,则也需要进行开颅术。血管膨胀(称为脑动脉瘤)也可以在开颅术期间修复。
要治疗不规则的血管形成(称为血管畸形),也可以进行开颅术。如果损伤或卒中引起脑水胀,开颅术可以释放脑部压力。
风险
开颅术的风险因手术类型而异。一般来说,风险可能包括:
- 颅骨形状改变。
- 麻木感。
- 嗅觉或视觉改变。
- 咀嚼时疼痛。
- 感染。
- 出血或血凝块。
- 血压变化。
- 癫痫发作。
- 无力以及平衡感出现问题或动作协调困难。
- 思维能力有问题,包括记忆丧失。
- 卒中。
- 脑内液体过多或肿胀。
- 脑和脊髓周围的液体渗出(称为脑脊液漏)。
罕见情况下,开颅术可能导致昏迷或死亡。
如何进行准备
医护团队会告诉您开颅术前需要做的事项。要准备进行开颅术,您需要接受几项检查,可能包括:
- 神经心理学测试。 这可以检测您的思维能力(称为认知功能)。结果作为基准,用于与后续检查进行比较,且有助于制定手术后的康复计划。
-
脑部影像学检查,比如 MRI 或 CT 扫描。 影像学检查可帮助医护团队制定手术计划。例如,如果手术是为了切除脑肿瘤,脑扫描可帮助神经外科医生看到肿瘤的位置的大小。也可能会通过 IV 的方式向手臂静脉注射造影剂。造影剂有助于在扫描中更清晰地显示肿瘤。
MRI 的一种,称为功能 MRI(fMRI),可以帮助外科医生绘制脑部各个区域。使用脑部特定区域时,fMRI 可显示血流的微小变化。这能够帮助外科医生避开控制重要功能(比如语言)的脑部区域。
饮食及药物
医护团队将提供手术前是否需要停止服用特定药物的说明。还会开具手术前需要服用的药物。该说明将告诉您开颅术前可以食用或饮用的食物。
-
用药改变。 手术前,告知医护团队您服用的任何药物或者对药物的任何过敏情况。其中包括需要处方药物和非处方药物。包括维生素、草本产品和其他补充剂。
如果服用糖尿病药物二甲双胍并在影像学检查中 IV 造影剂,则您可能出现副作用。为了避免出现这种情况,医务人员可能告诉您不要在注射造影剂后 48 小时内服用某些药物。具体决定取决于您的化验结果。
血液稀释药物影响凝血和出血。在手术之前,做手术的医务人员和管理药物的医务人员需要决定是否需要更改药物。安排好手术之后,请尽快咨询医护团队您要服用的药物。如果不确定是否服用血液稀释药物,请联系医护团队或药剂师。
您可能需要在手术前服用抗生素或其他药物。请咨询医护团队是否需要在手术前服用任何药物。
- 手术前可以食用或饮用的食物。 遵循医护团队关于手术前何时禁饮禁食的说明。
可能出现的情况
开颅术前可能会剃去头部毛发。大多数时候,您需要躺着进行手术。但是有时候需要俯卧、侧卧或保持坐姿。头部需要放在框架内。但是,3 岁以下的儿童在开颅术过程中没有头部框架。
如果患有称为胶质母细胞瘤的脑肿瘤,可能会为您提供荧光造影剂。该造影剂使肿瘤会在荧光灯下发光。这种光可帮助外科医生将其与其他脑组织分开。
手术时您可能会进入类似于睡眠的状态。这称为全身麻醉。或者,如果外科医生在手术期间需要检查脑功能,比如运动和语言功能,您可能会在部分手术过程中保持清醒。这是为了确保手术不影响重要的脑功能。例如,如果要进行手术的脑部区域靠近脑部语言区域,则会在手术过程中要求您说出物体的名称。
进行清醒手术时,您会在部分手术中保持类似于睡眠的状态,在部分手术中保持清醒状态。手术前,对要手术的脑部区域应用麻醉药。还会提供帮助您感觉放松的药物。
术中
开颅术过程中,神经外科医生切开颅骨上方的头皮,将皮肤折叠。外科医生使用手术钻头切入颅骨。暂时移除部分颅骨,以显示需要治疗的脑部区域。然后切开脑部外面的坚韧覆盖物,称为硬脑膜。有时外科医生需要做一个进入脑部的切口。
如果进行开颅术是为了提取组织样本进行检测(称为活检),则采集样本。如果正在接受脑肿瘤或血管畸形治疗,则外科医生将继续切除相关部分。如果患有动脉瘤,神经外科医生会使用血管夹阻断流向动脉瘤的血液。如果脑出血或者有血凝块,手术团队将在手术过程中清除血液。
手术期间可能使用的技术包括:
如果正接受脑肿瘤治疗,则手术目标是完全切除肿瘤。如果肿瘤靠近控制语言、运动或呼吸功能的脑部区域,外科医生可能无法完全切除肿瘤。如果留下部分肿瘤,手术后可能需要进行放射疗法或化疗。有时外科医生会在开颅术过程中将化疗或靶向放射放在脑中进行。
外科医生完成脑部手术之后,会将硬脑膜缝合在一起并密封。然后将移除的颅骨放回原位。金属螺钉、金属板、金属丝或缝线将其固定到位。金属材料通常由钛制成,因此未来可以进行 MRI 扫描。外科医生使用缝线或缝合钉使皮肤闭合。
术后
开颅术之后,从颅骨向外伸出一根小管。这是一根引流管,可让多余的液体从颅骨中流出。还可能会有其他导管来排出血液。引流管通常在大约三天后取下。
手术后大约 1 至 3 天,需要进行影像学检查,比如 MRI 扫描或 CT 扫描。此检查可以向外科医生显示肿瘤是否完全切除。
开颅术后,可能需要在医院恢复大约 4 到 6 天。住院时长因以下因素而异:手术原因、健康状况和是否需要进行其他治疗。
开颅术后完全康复可能需要几周。
如果服用血液稀释药物并在手术前停止服用这些药物,请咨询医护团队何时重新服用这些药物。因为某些常见的止痛药影响血液稀释,请咨询医护团队手术后疼痛时可以服用哪些药物。
结果
开颅术之后,您需要前往医护团队进行复诊。如果手术后出现任何症状,请立即告知医护团队。
您可能需要进行血液检查或影像学检查,比如 MRI 扫描或 CT 扫描。这些检查可以显示肿瘤是否复发或者是否仍然存在动脉瘤或其他状况。检查还可以确定脑部是否出现任何长期变化。
手术过程中,可能已将肿瘤样本送往实验室进行化验。化验可以确定肿瘤类型以及需要哪些后续治疗。
有些人需要在开颅术后接受放疗或化疗以治疗脑肿瘤。有些人需要二次手术以切除剩余肿瘤。
Long-term side effects of craniotomy
Sometimes, surgical scars can remain painful or sensitive for years after a craniotomy. This is often due to nerve endings trapped in scar tissue or chronic inflammation around titanium hardware. The pain may feel sharp, burning, tight or itchy.
These treatments for long-term scar pain after craniotomy may provide relief:
- Physical therapy. This helps you regain strength and movement and can reduce pain. It includes exercises, stretching, and using heat or cold.
- Scar massage. This involves gently rubbing the surgical scar to make it softer, more flexible and less sensitive. This can help with tightness, itching and overall comfort. It works by improving blood flow and breaking down stiff scar tissue.
- Medicines. These include those for nerve pain target pain coming from damaged nerves. Common examples include gabapentin and pregabalin, as well as certain antidepressants such as amitriptyline or duloxetine. Topical creams or patches with pain-relieving ingredients also can be used.
- Nerve blocks. These involve injecting numbing medicine near specific nerves to stop pain signals from reaching your brain. This can be very effective for headaches and other pain in the head and scalp.
- Removing hardware if it's the cause of pain. Though rare, the metal plates and screws used to put your skull back together after surgery can cause pain. If this is the case, removing these hardware pieces can help relieve the pain.
Other long-term side effects of craniotomy vary from person to person and depend on the type of surgery and recovery.
- Headache or sensitivity. Some people have ongoing headaches or a tight or odd feeling at the surgery site. This may be related to scarring, nerve irritation or changes in fluid pressure. In some cases, the discomfort can last for months or even years.
- Scalp or bone flap pain. Some people report long-term soreness or sharp pain near the incision. This can be caused by trapped nerves, tight scalp muscles, or sensitivity from plates or screws. When nerves are involved, this is called neuropathic pain.
- Numbness or tingling. Numbness around the incision is common, especially near the forehead, temple or behind the ear. It often fades with time but sometimes can last or feel unusual when touched.
- Seizures. Some people develop seizures after surgery, especially if brain tissue was affected. Long-term use of seizure medicines may be needed.
- Cognitive or emotional changes. Changes in memory, attention, mood or personality may occur if certain areas of the brain were involved. Fatigue or slower thinking can also happen during recovery.
- Infection or poor bone healing. Rarely, the bone flap doesn't heal well or becomes infected. This may require another surgery. Hardware used during the surgery also can shift or cause discomfort in some people.
Sept. 10, 2024